MRI FOR ALL

by ADRIAN CHO 23 FEB 2023
Hyperfine’s Swoop, the first U.S. FDA–approved low-field brain scanner, can be
wheeled to a patient’s bedside. DEREK DUDEK/HYPERFINE
The patient, a man in his 70s with a shock of silver hair, lies in the neuro intensive care unit (neuro ICU) at Yale New Haven Hospital. Looking at him, you’d never know that a few days earlier a tumor was removed from his pituitary gland. The operation didn’t leave a mark because, as is standard, surgeons reached the tumor through his nose. He chats cheerfully with a pair of research associates who have come to check his progress with a new and potentially revolutionary device they are testing.
The cylindrical machine stands chest high and could be the brooding older brother of R2D2, the Star Wars robot. One of the researchers carefully guides the 630-kilogram self-propelled scanner up to the head of the bed, steering it with a joystick. Lifting the man by his bed sheet, the researchers help him ease his head into the Swoop—a portable magnetic resonance imaging (MRI) scanner made by a company called Hyperfine.
“Do you want ear plugs?” asks Vineetha Yadlapalli, the second researcher.
“Is it as loud as a regular MRI?”
“Not at all.”
“Then I guess I don’t need them.”
After propping up the patient’s legs to ease the strain on his back, Yadlapalli sets the machine to work, tapping in a few instructions from an iPad. The machine emits a low growl, then proceeds to beep and click. Within minutes, an image of the patient’s brain appears on Yadlapalli’s tablet.
For a half-hour, the man lies quietly, hands folded across his belly. He could be getting his hair set in an old-fashioned hair dryer. In a small way, he’s a pioneer helping take MRI where it’s never gone before.
In many cases, MRI sets the gold standard in medical imaging. The first useful MRI images emerged in the late 1970s. Within a decade, commercial scanners had spread through medicine, enabling physicians to image not just bone, but soft tissues. If doctors suspect you have had a stroke, developed a tumor, or torn cartilage in your knee, they’ll likely prescribe an MRI.
If you’re fortunate enough to be able to get one, that is. An MRI scanner employs a magnetic field to twirl atomic nuclei in living tissue—specifically the protons at the heart of hydrogen atoms—so that they emit radio waves. To generate the field, a standard scanner employs a large, powerful superconducting electromagnet that pushes a machine’s cost to $1.5 million or more, pricing MRI out of reach of 70% of the world’s population. Even in the United States, getting an MRI may require days of waiting and a midnight drive to some distant hospital. The patient must come to the scanner, not the other way around.
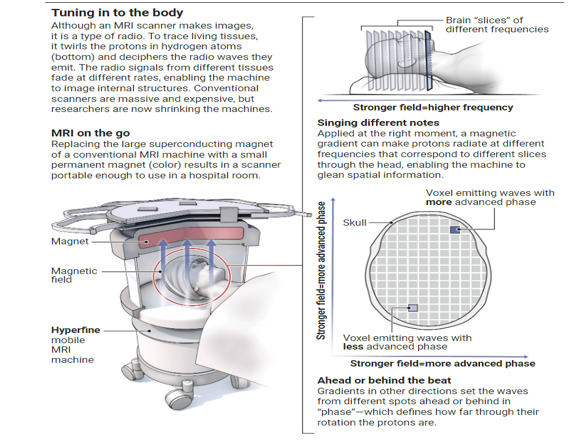
For years, some researchers have been striving to build scanners that use much smaller permanent magnets, made of the alloy often found in desk toys. They produce fields roughly 1/25th as strong as a standard MRI magnet, which once would have been far too weak to glean a usable image. But, thanks to better electronics, more efficient data collection, and new signal processing techniques, multiple groups have imaged the brain in such low fields—albeit with lower resolution than standard MRI. The result is scanners small enough to roll to a patient’s bed and possibly cheap enough to make MRI accessible across the globe.
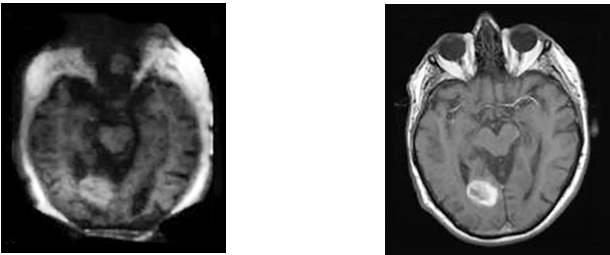
The resolution of a brain scan from a low-field machine (first image) is coarser than conventional MRI (second image), but both images clearly reveal a hemorrhage. YALE SCHOOL OF MEDICINE
The machines mark a technological triumph. Kathryn Keenan, a biomedical engineer at the National Institute of Standards and Technology who is testing a Hyperfine scanner, says, “Everyone that comes through is super impressed that it even works.” Some say the scanners could also transform medical imaging. “We’re potentially opening up a whole new field,” says Kevin Sheth, a neurologist at the Yale School of Medicine who has worked extensively with the Swoop but has no financial interest in Hyperfine. “It’s not a question of ‘Is this going to happen?’ It’s going to be a thing.”
In August 2020, the Swoop became the first low-field scanner to win U.S. Food and Drug Administration (FDA) approval to image the brain, and physicians are putting it through clinical studies at Yale New Haven and elsewhere. Other devices are close behind. But Andrew McDowell, a physicist and founder of the consulting firm NeuvoMR, LLC, cautions it’s not clear there’s a market for a low-field scanner, with its lower resolution. “The real challenge is going to be convincing doctors to start using it,” he says. “That’s very difficult because for good reasons they’re very conservative.”
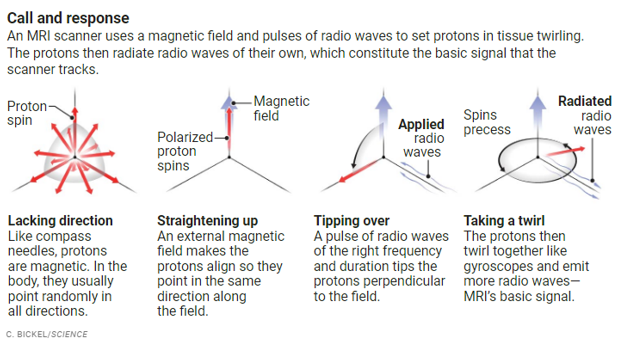
AN MRI SCANNER WORKS nothing like a camera; it is actually a radio that tunes in to protons in living tissue. Like a tiny compass needle, each proton is magnetic, and ordinarily the protons point randomly in all directions (see graphic, below). However, an external magnetic field can align them. At that point, a pulse of radio waves of the right frequency and duration can tip them by 90°. The aligned protons then twirl like gyroscopes, emitting a radio signal of their own, whose frequency increases with the field’s strength.
That fleeting monotone radio hum reveals little. To create an image, the scanner must distinguish among waves coming from different points in the body. To do this, it sculpts the magnetic field, which makes protons at different locations sing at different frequencies and states of synchrony. The scanner must also distinguish one type of tissue from another, which it does by exploiting the fact that the radio signals fade at different rates in different tissues.
One reason the signal dies out is that the protons knock one another out of alignment through their own magnetic fields. The rate at which this happens differs between, say, fatty brain matter and watery cerebrospinal fluid. To measure the rate, the scanner applies pairs of pulses. The first pulse creates a signal that fades as the orientations of twirling protons fan out. The second reverses much of that evolution, eliciting an echo of the signal. The proton-proton interactions mute that echo, however. So the scanner can measure their rate by tracking how the echo shrinks as the delay between the two pulses increases.
While applying pair after pair of pulses, the scanner must simultaneously sort the echoes coming from different points in the brain. To do that, it relies on magnetic field gradients applied at key moments. For example, a gradient applied during the echo from chin to crown makes protons in different sideways slices through the head radiate at different frequencies. A gradient applied between pulses and across the head will set protons in vertical slices ahead or behind in their twirling, a “phase” difference that makes echoes from some slices reinforce one another and others cancel. By varying the gradient, the scanner can deduce the strength of the echo from each slice.
Over many repetitions, the scanner gathers a plethora of echoes in which intensity varies with delay, frequency, and phase. A standard mathematical algorithm decodes them to produce a map of how the proton-proton interactions vary throughout the brain, forming one type of MRI image. Other pulse sequences probe other tissue-specific processes—such as how fast protons diffuse, which can track fluid flow.
All that pulsing explains why MRI scans take time and why an MRI machine chirps, clicks, and buzzes. Those sounds emerge as mechanical stresses rattle the current-carrying coils that create the magnetic gradients. A technician can tell what kind of a scan a machine is doing just from those sounds, Yadlapalli says.
A stronger field makes all this easier by polarizing the protons more thoroughly and creating a bigger signal. A standard scanner’s magnet produces a field of 1.5 tesla—30,000 times as strong as Earth’s field—and some reach 3 or 7 tesla. Even so, the protons pointing along a 1.5-tesla field outnumber those pointing the other way by just 0.001%. Reduce the field strength by a factor of 25 and the polarization falls with it. The signal-to-noise ratio plummets even more, by a factor of nearly 300.
In principle, a low-field scanner could coax a signal from the noise by taking data over a longer time period—just as radio astronomers sift a weak signal from noise by training their dishes on a star for hours or days. That tack won’t work with a human, who can hold still only so long. So, in developing low-field MRI, researchers had to find ways to extract data much faster.
One key element is better hardware, says Joshua Harper, a neural engineer at the German Paraguayan University. “We now have really fast, really cheap electronics,” he says. “That’s really why it works.” Even so, doing low-field MRI in a hospital room is tricky. Metal in other machines and even the walls can distort the field, and static from other devices can disrupt the radio signal. So, scanners employ countermeasures. For example, Hyperfine’ s Swoop uses antennas to measure radio noise and cancel it, similar to how noise-canceling headphones block sound.
The new scanners also turn an aspect of the lower field to their advantage to run faster. To manipulate the protons, a high-field scanner must use higher frequency, higher energy radio waves, so it can pulse only so fast before it begins to heat the patient. Free of that speed limit, a low-field scanner can pulse faster and use more efficient pulse sequences, says Matthew Rosen of Massachusetts General Hospital, a physicist who co-founded Hyperfine. “We can interrogate very, very rapidly, doing things that you could never do at high field.”
Even so, gathering data fast enough for standard image reconstruction remains a challenge. One solution is to employ novel signal processing techniques, including artificial intelligence. Hyperfine engineers use a set of training images to teach a program called a neural network to construct brain images from relatively sparse data, says Khan Siddiqui, Hyperfine’ s chief medical officer and chief strategy officer. “That’s where our secret sauce comes in.”
Compared with a standard scan, a low-field image looks blurrier. Still, physicists see its beauty. “It’s this incredible physics success story,” Rosen says. “It’s not just we pointy headed physicists [goofing] off and doing stuff that nobody cares about.” The technology vindicates those toiling in a forgotten corner of the field, McDowell says. “Who in their right mind would build a 65-millitesla machine when the glory is in building the 11-tesla one?”
HYPERFINE SAYS ITS SWOOP SCANNER is off to a pretty glorious start. It has sold more than 100 of the machines, mostly in the United States, at about $250,000 apiece. The goal is not to replace high-field scanners, but to expand how MRI is used, Siddiqui says. “Our portable scanner brings MRI closer to the patient, both in time and in distance.” Hyperfine envisions using it in the neuro ICU to quickly assess patients too ill or unstable to wheel to a conventional MRI or a CT machine, which produces a type of 3D x-ray.
A Swoop’s magnet consists of two disks and produces a field of 64 millitesla. A scan from it feels dramatically different from a standard scan. In a conventional scanner, an automated table glides you bodily into the cylindrical magnet. With the Swoop, an able patient can scooch into the magnet as if wriggling under a car’s bumper. A helmetlike head piece containing the antennas cradles your head so snugly it may touch your nose, yet your arms and legs are free. The machine’s chirping is soft, even soothing.
In late 2019 and early 2020, as the coronavirus pandemic took hold, Sheth and colleagues tested the Swoop’s promise by scanning 50 ICU patients, including 20 with COVID-19. Because many were on ventilators and sedated, “we had no idea what their neurological status was and no way to take a look by any available imaging modality,” Sheth recalls. “And this provided us a way to do that at the bedside.” The scans revealed brain trauma in 37 cases, including eight COVID-19 patients, the researchers reported in January 2021 in JAMA Neurology.

A low-field MRI scanner images a patient in their bed in the intensive care unit at Yale New Haven
Hospital. YALE SCHOOL OF MEDICINE
The cheaper, smaller machines might also allow patients to get more frequent follow-up scans. That’s a prospect that resonates with Ronald Walsworth, a physicist at the University of Maryland, College Park, and co-founder of Hyperfine. In 2007, his then–2-year-old son developed a noncancerous brain tumor. He was treated successfully, says Walsworth, who serves on Hyperfine’s advisory board. Still, he says, “There were signs that were not caught early and things that were not decided most efficiently because the MRIs only could happen once in a while.”
The Swoop’s advantages have won it fans. “Oh, my God, what a beautiful, beautiful piece of technology,” says Steven Schiff, a pediatric neurosurgeon at Yale University who has no financial interest in Hyperfine. Still, the Swoop can miss details a high-field scanner would catch because its resolution of 1.5 millimeters is half that of a standard scanner. For example, Sheth’s team used it to image the brains of 50 patients who had had an ischemic stroke, visible with standard MRI. The Swoop missed the five smallest, millimeter-size strokes, the researchers reported in April 2022 in Science Advances.
That finding shows physicians will have to exercise judgment in deciding when to use each type of scanner, Sheth says. “You shouldn’t be too worried, but you should understand the context in which you might miss something,” he says. Still, McDowell notes doctors may shy away from a low-field scanner if they think using it could leave them open to a malpractice suit.
IN MUCH OF THE WORLD, MRI is simply unavailable. A team in the Netherlands hopes its scanner will change that. Its magnet differs dramatically from the Swoop’s. It consists of 4098 cubes of neodymium iron boron—an alloy developed in the 1980s by carmakers—embedded in a hollow plastic cylinder, and arranged in a configuration called a Halbach array to produce a uniform horizontal field. “Our system is intrinsically better and has fewer distortions,” asserts Andrew Webb, an MRI physicist at Leiden University Medical Centre, so it requires less help from processing such as machine learning.
A private company, Multiwave Technologies in Switzerland, is trying to bring the scanner to market. It will apply for FDA approval this year and aims to rent its machines in a subscription model, says Tryfon Antonakakis, Multiwave’s co-CEO. “Our goal is to make it as affordable as possible and not necessarily to be in the hospital,” says Antonakakis, an engineer and applied mathematician. “We are looking to go into the mountains, into the medical deserts in developing countries.”
Webb and his colleagues, including Martin van Gijzen, an applied mathematician at the Delft University of Technology, have another plan for spreading their technology: giving it away. “We made the decision—Martin, myself, all our team—that we were not going to patent things,” Webb says. “Everything is going to be open source,” so that anyone can download their design from the internet and build scanners. Webb and colleagues hope entrepreneurs in developing nations will manufacture them locally.
To seed the idea, they shipped a scanner, packaged as a kit, to Johnes Obungoloch, a biomedical engineer at Mbarara University of Science and Technology in Uganda, who was a graduate student at Pennsylvania State University, University Park, when Webb and Schiff were also there. In September 2022, Webb and others flew to Uganda to help Obungoloch and his team assemble the scanner in 11 days.

Soon it will be put to use in a project to test the utility of low-field MRI in the developing world. The CURE Children’s Hospital of Uganda, a 55-bed pediatric neurosurgical facility in Mbale run by an international nonprofit, plans to compare Obugoloch’s scanner, a Swoop, and a CT scanner. Doctors will image children with hydrocephalus, in which cerebrospinal fluid collects in the brain and compresses it, potentially causing debilitating or fatal damage. Globally, hydrocephalus afflicts 400,000 children every year, and it accounts for 75% of the CURE hospital’s patients. In Africa, an infection is the usual cause..For years, Schiff and colleagues at the hospital have used CT scans to guide an innovative surgery that allows the fluid to drain into the brain’s ventricles—an alternative to installing a shunt to the abdomen. However, a CT scan exposes children to considerable x-ray radiation, so CURE doctors will see whether low-field MRI images can guide surgeons. “If the MRI proves comparable to the CT scan, then there is no reason why we should be using the CT scan anymore,” says Ronald Mulondo, a physician at CURE who directs the project.
The study is awaiting final governmental approval. If it’s successful, Obungoloch envisions building more scanners, perhaps for Africa’s six other CURE hospitals, and even sourcing some of the parts locally. Uganda has public health care, so that vision depends on government funding, he says.
Still, like their peers elsewhere, doctors in Uganda may have reservations about the technique’s limited resolution, Obungoloch notes. “The radiologists see it and say, ‘Well, this is a crappy image, and we don’t care how long it took you to acquire it.’” Government officials may also think Ugandans shouldn’t have to settle for lower resolution imaging, no matter how useful, he says.
In truth, developers of low-field MRI are pushing for nothing less than a rethink of medical imaging. “Is the best technology the scanner that can provide the highest quality images or is it the scanner that can lead to the most improved patient outcomes?” asks Harper, who collaborated on Webb’s open-source rig and hopes to acquire a Swoop.
What will win over doctors, Sheth says, will be a “use case”—a killer app for the scanners. For example, they might be put into special ambulances for stroke care. He questions whether Hyperfine and others have found that use case but predicts it will come.
file:///C:/Users/Owner/AppData/Local/Temp/msohtmlclip1/01/clip_image017.jpg" alt="Adrian Cho" width="86" height="120" />Then there are patients to win over. After his time in the Hyperfine scanner, the pituitary tumor patient confides to Yadlapalli that it wasn’t quite as comfortable as a regular MRI. Noting that he still can’t breathe through his nose because of the surgery, he says the snug-fitting head basket bothered him. “I’d rather be scooted over to a real MRI.” Call him a reluctant pioneer.
ABOUT THE AUTHOR
Adrian Cho, Author, Staff Writer
TRIZ Notes: This new MRI system has been reduced in size, weight, do it in reverse and convenient to use. The system is more IDEAL and will continue to evolve closer to the IFR. Just needs a few more “S” curves.